Hello!
My name is Urmi Mota and I’m a senior at BASIS Scottsdale. Instead of attending school for the last trimester, seniors at our school are given the unique opportunity to conduct a research study of their choice. I will be pursuing my Senior Project, “Within the NICU: It’s a Family Matter” at Banner Desert Medical Center, specifically in the NICU (Neonatal Intensive Care Unit) of the connected Cardon Children's Medical Center.
Ever since I was little, I’ve had an interest in medicine. No one in my immediate or extended family ever had a career in the medical field which is probably one of the main reasons that my curiosity for the field grew. Over the years, I have volunteered at multiple hospitals and participated in numerous classes both in and out of school that have helped me gain perspective about this field. Therefore, when the chance arrived where I could pursue a project of my choice, I knew that I wanted to explore this field, but I didn’t know what exactly I wanted to research. That is, until I started volunteering at Banner Desert Medical Center (BDMC).
 |
| Banner Desert Medical Center |
I became a hospital volunteer for BDMC in the fall of 2016, supervising those who enter and exit the NICU facility. Over the few months that I volunteered there, I wanted to learn more about what was going on within the NICU facility rather than just from the conversations I’ve had with people from the outside.
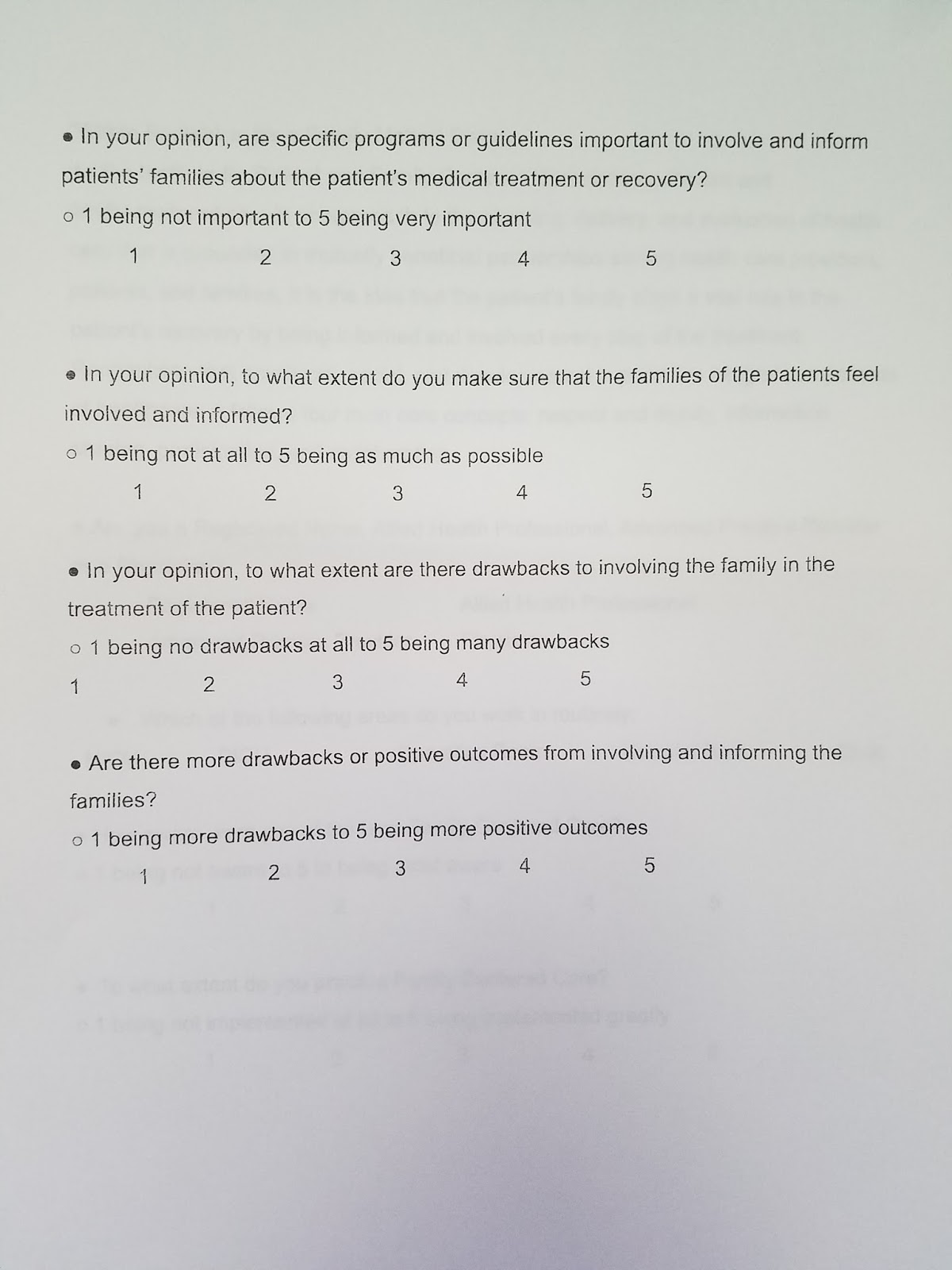
Family Centered Care, an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care providers, patients, and families, is the idea that the patient's family plays a vital role in a patient recovery by being informed and involved every step of the treatment. Before the 1970's, pediatric patients were often separated from their parents for diagnosis or treatment because of the belief that the hospital institution, treatment, and medication were the most important factors to improve a child’s health. In the 1970s and 1980s, the importance of family in pediatric health became more widely recognized and implemented. However, the implementation of family involvement in a child’s health progression was slower in the NICU compared to other medical services. While virtually all hospitals emphasize the importance of family interaction within pediatric patients’ road to recovery, some still restrict family involvement within the NICU with rules such as visiting hours or limits on external visitors other than immediate family members.
My research aims to look at to what extent Family Centered Care is implemented within the NICU at Banner Desert Medical Center. For a more detailed explanation of my project, please feel free to check out Senior Project Proposal on the right sidebar.
Along with shadowing neonatal professionals, neonatal nurses, and nurse practitioners here in Arizona, I hope that sometime in the next ten weeks that we spend pursuing this Senior Project I will be able to travel to India to observe to what extent Family Centered Care is implemented at the Shrimad Rajchandra Hospital in Dharampur, India. As this hospital is located in rural India, it would be very interesting to see to what extent the core ideas of Family Centered Care are implemented there, as the culture is completely different.
Over the next few months, I will update this blog regularly with my experiences and interesting findings I have while at the hospital. With only another week of school left, I am eager to start on this journey and hope that you come back to see where it takes me!